
Contributors
The Data is Clear: Covid mRNA Vaccination Does Not Protect Against Severe Hospitalization And Death
In this article, Dr. Pierre Kory compiles data showing that the vaccinated fared worse in the hospital, taken largely from non-U.S data because the U.S data is corrupted.

This article originally appeared on Dr Pierre Kory’s Substack and was republished with permission.
Guest post by Dr. Pierre Kory
The point of the article which references these data is to show the U.S data is corrupted.
**The data below are not comprehensive or up-to-date, but I believe sufficient to prove my point. Taken from posts I wrote in June and August of 2022. I long ceased to track such data, not only because, in my mind, the vaccines were already proven and dangerous failures, but also because many national health services ceased posting data which allowed us to compare the fates of the vaccinated and unvaccinated (thinking of you ONS and Scotland).

EFFICACY OF COVID VACCINES IN PROTECTION FROM SEVERE DISEASE
CDC data shows that there is no statistically valid evidence that they prevent severe disease or deaths in children. Current mRNA injections were formulated based on the original Wuhan strain and were not tested for benefits against current variants in clinical trials. Which begs the question as to what can be accomplished by vaccinating small children with an outdated vaccine.
In Ireland, in March of 2022, during the milder Omicron variant wave, there were more people in Irish hospitals than at any point in the previous 12 months. This occurred despite the fact that nearly 95% of all adults in Ireland are fully vaccinated, and nearly 100% of seniors are vaccinated and boosted.
In Scotland, on page 29 of their recent national COVID-19 report, the data revealed that the vaccinated were dying and being hospitalized at higher rates than the unvaccinated. Note that Scotland has since made the decision to no longer publish these comparative data for “concerns that they are being misinterpreted”. Although it is true, as I noted above, that numerous variables beyond vaccination status may contribute to explaining these differences, I find it troubling (similar to the Department of Defense actions mentioned above) that the decision to stop publishing these data occurred only after a negative efficacy against severe disease and death was found.
In Israel, the Director of a major hospital recently declared that the fully vaccinated are not protected against severe illness.
NSW Health in New South Wales, the most populated of Australian states at 8.1 million inhabitants, reported that 97 out of 98 COVID-19 deaths occurring over the previous two weeks involved fully vaccinated persons. Moreover, those that had three doses appeared most at risk for hospitalization admission, ICU transfer, and death.
These data are consistent with the recent report published in the New York Times which stated “despite strong levels of vaccination among older people, COVID killed them at vastly higher rates during this winter’s Omicron wave than did last year, preying on long delays since their last shots and the variant’s ability to skirt immune defenses.” I must add that these higher rates of death in the elderly are also seen in the boosted.
The conclusion of a recent Danish study in the prestigious Lancet found that in long-term follow-up of over 74,000 adult participants in the Moderna and Pfizer trials there was no all-cause mortality benefit from the two mRNA shots.
In a recent, large Veterans Administration study, investigators discovered disturbing evidence: by month six after a SARS-CoV-2 infection, beyond the first 30 days of illness, vaccinated persons with breakthrough infections were at higher risk of death (hazard ratio (HR) = 1.75, 95% confidence interval: 1.59,1.93).
NATURAL IMMUNITY
For those with natural immunity already, the data in support of further vaccination is even worse: The most recent review of data supporting the protection of natural immunity, compiled from over 150 research studies, found that natural immunity provided equal or superior protection against not only contracting the disease, but also against hospitalization and death.
Further, vaccinated individuals are far more likely to get re-infected with COVID compared to those with natural immunity. A new preprint study from Bangladesh found that among 404 people re-infected with COVID, having been vaccinated made someone 2.45 times more likely to get re-infected with a mild infection, 16.1 times more likely to get a moderate infection, and 3.9 times more likely to be re-infected severely, relative to someone with prior infection who was not vaccinated. Although overall re-infections were rare, vaccination was a greater risk factor of re-infection than co-morbidities.
A new study from Harvard, Continued Effectiveness of COVID-19 Vaccination among Urban Healthcare Workers during Delta Variant Predominance, tracked vaccinated and unvaccinated Massachusetts healthcare workers and showed 0 infections in 74,557 person-days for previously infected patients compared to 49 infections out of 830,084 person-days for fully vaccinated patients.
A study published in the New England Journal of Medicine assessed a cohort of 1,304 patients meeting a very strict definition of “re-infection.” In this cohort, there were no deaths and no ICU admissions during reinfections while 7 deaths and 28 ICU admissions occurred during the primary infections. Overall, there was a statistically significant 90% reduction in the composite outcome of severe, critical, or fatal disease during reinfections. Further, amongst all ages, CDC found that natural immunity offerred equal protection against hospitalization.
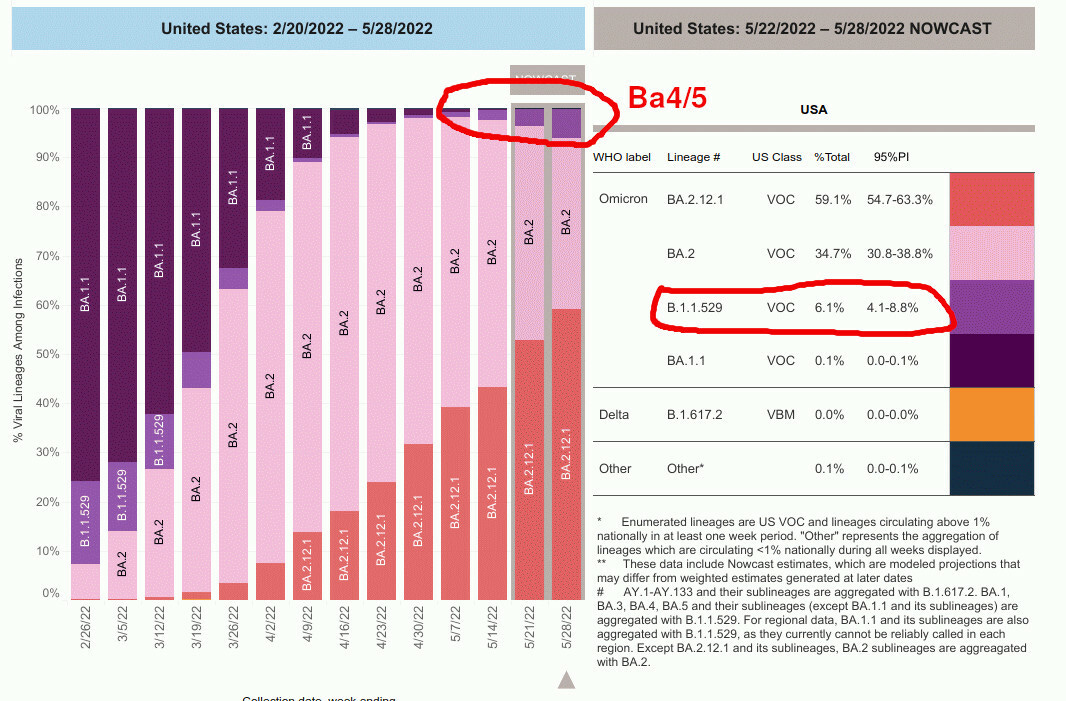
Thus, in terms of benefits, based on the most up-to-date data, the current crop of mRNA vaccines against Omicron confer either rapidly waning efficacy or negative efficacy, and not only do they no longer protect against severe disease, my interpretation of these data is that they appear to be raising the risk of severe disease and death. I would advise extreme caution given that, currently, in the U.S, the prevalence of the B4/5 variant appears to be doubling every week in the past month, now comprising approximately 8% of cases.
In regards to the current variant B4/5, my rapidly evolving clinical experience and those of my network of colleagues is that the vaccinated are contracting more severe illness and are less quickly responding to combination anti-viral and anti-inflammatory therapies.
Copyright 2024 Dr. Pierre Kory











{kind=link}

New CDC Report Denies Link Between COVID Shots and Sudden Deaths in Young Adults

Supreme Court Justice Drops a Bomb on DOJ’s Case Against J6 Protesters

High School Student Suspended for Saying “Illegal Alien”

Lawsuits by Detransitioners Skyrocket as Transgender Movement Retreats

“We Have 15,000 Samples In Wuhan … Could Do Full Genomes of 700 CoVs”: Rand Paul Drops COVID Bombshell

Confirmed: COVID mRNA Vaccines Contain Component that Suppresses Immune Response and Stimulates Cancer Growth

Boeing Whistleblower Says ENTIRE FLEET of 787s Should Be Grounded Worldwide

Dr. McCullough Issues Major Bird Flu Warning: “A Perfect Storm Is Brewing”

The Real Dangers of Biden’s Hidden Tax on All Americans

What Have Vaccines Done to Us? The Truth is Disturbing

Russell Brand Goes Quiet as Florida Surgeon General Drops a Bomb on Dr. Anthony Fauci

New WEF Report Reveals the Global Elites’ Shocking Plan to Enforce Vaccination

Nikki Haley Reveals Her New Job After Dropping Out of 2024 Presidential Race in Disgrace

Why You Should Never, Ever Voluntarily Talk to the FBI

Bishop Viciously Stabbed During Church Service in Sydney Just Days After Mall Massacre

The WHO Wants Sweeping Global Power Over Pandemic Policy — Without Defining ‘Pandemic’
Confirmed: COVID mRNA Vaccines Contain Component that Suppresses Immune Response and Stimulates Cancer Growth
Boeing Whistleblower Says ENTIRE FLEET of 787s Should Be Grounded Worldwide
Supreme Court Justice Drops a Bomb on DOJ’s Case Against J6 Protesters
Boeing Whistleblower Says ENTIRE FLEET of 787s Should Be Grounded Worldwide

Neocon Nikki Haley Reveals New Job After Dropping Out of 2024 Presidential Race in Disgrace

Corrupt Judge Issues Cold-Blooded Threat to President Trump
Russell Brand Goes Quiet as Florida Surgeon General Drops a Bomb on Dr. Anthony Fauci

Dr. Phil Show Exposes High-Tech Chinese Military Ops Inside America Near US Military Bases

Dr. Peter McCullough Gives a Masterclass in How to Debate COVID Vaccine Safety with Democrats

Dr. Peter McCullough Sounds the Alarm on COVID Vaccine-Induced “Turbo Cancer”

NPR Senior Editor Suspended After Blowing Whistle on Network’s Bias Coverage
-
 Health2 days ago
Health2 days agoWhat Have Vaccines Done to Us? The Truth is Disturbing
-
 Health22 hours ago
Health22 hours agoRussell Brand Goes Quiet as Florida Surgeon General Drops a Bomb on Dr. Anthony Fauci
-
 Health3 days ago
Health3 days agoNew WEF Report Reveals the Global Elites’ Shocking Plan to Enforce Vaccination
-
 News1 day ago
News1 day agoNikki Haley Reveals Her New Job After Dropping Out of 2024 Presidential Race in Disgrace